For most of the modern history of incretin science, the design goal was singular: activate the GLP-1 receptor, and do it for longer than the natural hormone manages. The more interesting question, and the one that now drives much of the field, is what happens when a single molecule is designed to engage more than one incretin receptor at the same time.
The Two Incretin Receptors
Incretins are gut hormones released in response to food that signal to the pancreas and the brain. Two matter here.
GLP-1 — glucagon-like peptide-1 — is the better-known of the two. Activity at its receptor is associated with glucose-dependent insulin secretion, suppression of glucagon, slowed gastric emptying and satiety signalling in the brain.
GIP — glucose-dependent insulinotropic polypeptide — is the other major incretin, and its story is stranger. GIP is actually the more abundant incretin in healthy physiology, but its insulin-stimulating effect appears blunted in type 2 diabetes, which for years led the field to largely set it aside as a target. Renewed interest came from the observation that when GIP signalling is combined with GLP-1 signalling, the receptor's contribution looks different than it does in isolation.
Single Agonists Versus Dual Agonists
A single incretin peptide — a GLP-1 receptor agonist — engages one receptor. This is a well-characterised class with a long evidence base in glucose regulation and body weight.
A dual incretin peptide — a GIP/GLP-1 receptor agonist — is engineered as one molecule that binds both receptors. It is not two compounds in a vial; it is a single peptide backbone designed so that different regions of the same chain interact with two different receptors, with deliberately tuned potency at each.
That last point is the part worth appreciating. The design question is not merely "can it hit both?" but "in what ratio?" A dual agonist can be balanced, or biased toward one receptor, and the balance is a design decision with real consequences. This is protein engineering at a level of control that would have been unrealistic a couple of decades ago.
Beyond dual agonists, the same logic extends further. Triple agonists — engaging GIP, GLP-1 and the glucagon receptor — are under active investigation, on the reasoning that glucagon signalling may contribute to energy expenditure. That work is at an earlier stage and should be read as such.
How a Head-to-Head Comparison Is Built
Comparing two active compounds directly is a much stronger evidential design than comparing each to placebo separately and eyeballing the gap.
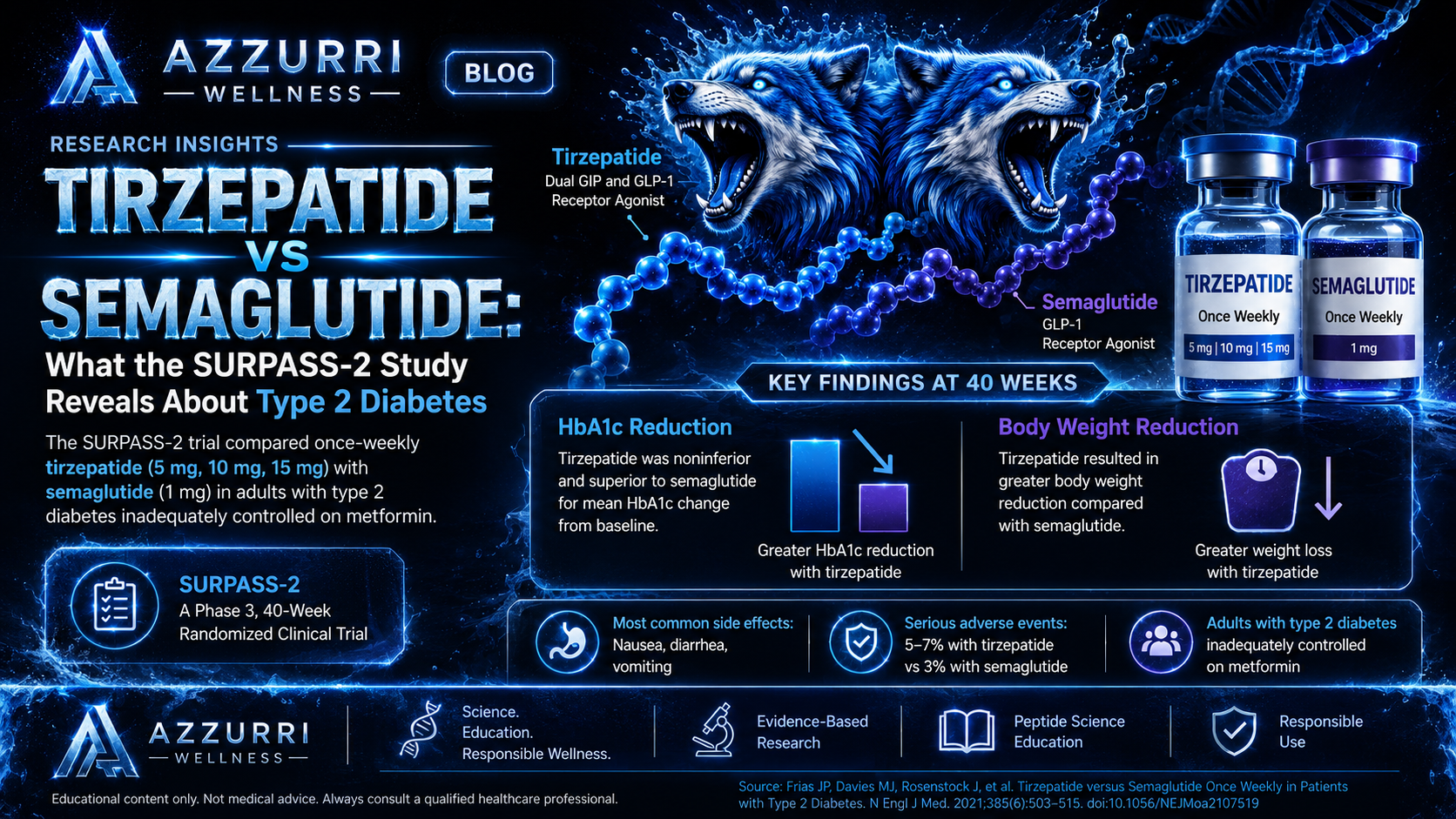
Population. Adults with type 2 diabetes whose glucose control is inadequate on an existing baseline therapy, commonly metformin. Studying people on a stable background therapy isolates the effect of the compound being added.
Design. Participants are randomised to one compound or the other, with the comparison typically run across several strength levels so that the response can be characterised rather than reduced to a single point.
Primary endpoint. Change in HbA1c from baseline. HbA1c reflects average blood glucose over the preceding two to three months and is the standard metric for glucose control in diabetes research, precisely because it is not distorted by what someone happened to eat that morning.
Statistical structure. These comparisons are typically framed first as a non-inferiority test — is the new compound at least not meaningfully worse — with superiority testable only if non-inferiority is established. This hierarchy is set out in advance, which is what prevents a trial from fishing for a favourable result after the fact.
What a Comparison Result Establishes
A head-to-head trial establishes how two compounds performed relative to each other, on defined endpoints, in a defined population, over a defined period.
It does not establish which is "better" in any general sense. That framing collapses several things a single trial cannot resolve: the comparison is made at particular strength levels and would not necessarily hold at others; tolerability trades off against effect on the primary endpoint, and different people weigh that trade differently; and glucose control, body weight and side-effect burden are separate outcomes that a single ranking cannot capture.
Safety and Tolerability
Across incretin-based compounds, the dominant adverse events are gastrointestinal: nausea, diarrhoea and vomiting. In trial reports they are typically described as mild to moderate and as most pronounced early on.
A general pattern in this literature is that greater effect on metabolic endpoints tends to come with a greater burden of gastrointestinal side effects. That trade-off is a large part of why these compounds are used under supervision — someone has to monitor how a given person is actually tolerating them.
What This Says About Peptide Engineering
Natural peptide hormones are short-lived by design; the body wants signals that switch off. Modern incretin peptides are engineered against that grain — modified for stability, tuned for receptor selectivity, and in the dual-agonist case built to carry two signals on one backbone.
The single-versus-dual comparison is therefore a useful window into where peptide science currently sits: it is no longer only about making a natural signal last longer, but about deciding which combination of signals to send.
A quick, important note
Our products are prepared by a Registered 503B outsourcing facility and provided under physician guidance. This article is here to educate, not to replace medical advice. Your physician should be the one guiding whether any peptide is appropriate for your situation.

