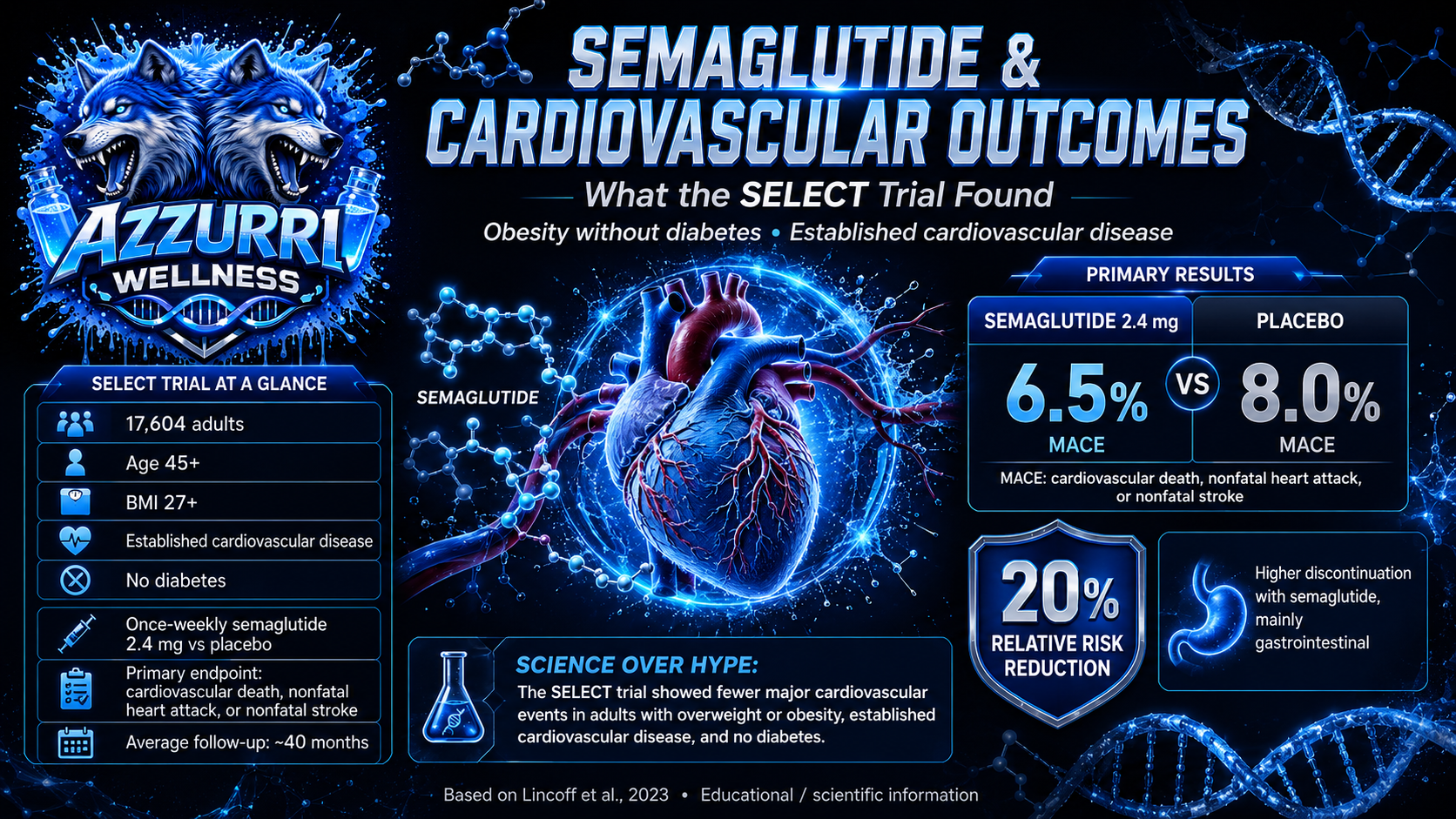
Semaglutide is widely associated with blood-glucose control and weight management. The SELECT trial asked a different and clinically important question: Could semaglutide reduce major cardiovascular events in people with overweight or obesity who already had cardiovascular disease but did not have diabetes? Published in The New England Journal of Medicine in 2023, SELECT was a large, randomized, double-blind, placebo-controlled trial involving 17,604 adults. The results showed fewer major cardiovascular events among participants assigned to semaglutide than among those receiving placebo. Who participated in SELECT? Participants were at least 45 years old and had: A body-mass index of 27 or higher Established cardiovascular disease No previous diagnosis of diabetes Established cardiovascular disease included previous myocardial infarction, stroke, or symptomatic peripheral arterial disease. Participants were randomly assigned to receive either once-weekly subcutaneous semaglutide, targeted at 2.4 mg, or placebo alongside their usual cardiovascular care. This was therefore a secondary-prevention trial. It studied people who already had cardiovascular disease—not healthy individuals seeking to prevent their first cardiovascular event. What was the primary outcome? The primary endpoint was a composite known as major adverse cardiovascular events, or MACE. It included: Death from cardiovascular causes Nonfatal heart attack Nonfatal stroke During an average follow-up of approximately 40 months, a primary cardiovascular event occurred in: 6.5% of participants receiving semaglutide 8.0% of participants receiving placebo The hazard ratio was 0.80, corresponding to a 20% relative reduction in the risk of the combined endpoint. The absolute difference between the groups was 1.5 percentage points. Why was the result important? Previous cardiovascular-outcome trials had shown benefits from GLP-1 receptor agonists in people with type 2 diabetes. SELECT demonstrated that cardiovascular benefit could also be observed in a population without diabetes, provided participants had overweight or obesity and established cardiovascular disease. The findings should not be simplified to mean that semaglutide prevents every heart attack or stroke. The result applies to the combined probability of three cardiovascular outcomes within the trial’s defined population and follow-up period. It is also important to distinguish between relative and absolute effects: The relative risk reduction was approximately 20%. The observed event rates differed by 1.5 percentage points. Both numbers are accurate, but they communicate different aspects of the result. Was the benefit caused only by weight loss? SELECT established that semaglutide reduced cardiovascular events, but the original trial was not designed to prove one single mechanism. Potential contributors may include changes in: Body weight Blood pressure Glucose regulation Inflammation Lipid metabolism Vascular or cardiac biology The trial’s cardiovascular result should therefore not be presented as proof that weight loss alone caused the observed benefit. Later prespecified SELECT analyses have continued investigating the relationship between weight change and cardiovascular outcomes. What did the trial show about safety? Serious adverse events were reported in 33.4% of the semaglutide group and 36.4% of the placebo group. However, adverse events leading to permanent discontinuation were more frequent with semaglutide: 16.6% with semaglutide 8.2% with placebo Gastrointestinal complications were an important reason for discontinuation and occurred more frequently in the semaglutide group. This distinction matters. A treatment can reduce the risk of a major clinical outcome while still causing tolerability problems for some participants. What SELECT does not prove The findings should not automatically be applied to: People without established cardiovascular disease Adults with a BMI below the trial threshold People with diabetes Younger populations Unregulated or non-pharmaceutical semaglutide products Different doses or administration methods Short-term or occasional use SELECT studied a specific regulated formulation, administered once weekly under clinical-trial conditions and added to standard cardiovascular care. The trial also does not show that semaglutide replaces established cardiovascular treatments such as lipid management, blood-pressure treatment, antiplatelet therapy when indicated, smoking cessation, nutrition, or physical activity. Study strengths and limitations Strengths Large sample of more than 17,000 participants Randomized, double-blind design Placebo comparison Long cardiovascular follow-up Clinically meaningful endpoint Inclusion of participants from multiple countries Limitations The trial only enrolled people with established cardiovascular disease and excluded diabetes. Its findings therefore address secondary cardiovascular prevention in a defined high-risk population rather than cardiovascular prevention for everyone with overweight or obesity. Treatment discontinuation was also more common with semaglutide, particularly because of gastrointestinal adverse effects. The study was funded by Novo Nordisk, the manufacturer of semaglutide, and this funding relationship should be disclosed when interpreting and communicating the findings. The Azzurri Wellness perspective SELECT demonstrates why semaglutide research should be evaluated through clearly defined outcomes rather than general marketing statements. The trial did not simply measure changes on a scale. It measured cardiovascular death, nonfatal heart attack, and nonfatal stroke in a large population with established cardiovascular disease. Its central finding was significant but specific: In adults with overweight or obesity, established cardiovascular disease, and no diabetes, once-weekly semaglutide reduced the risk of major adverse cardiovascular events compared with placebo. Responsible scientific communication must include the population studied, absolute event rates, treatment duration, adverse effects, and limitations—not only the headline percentage.
References Lincoff AM, Brown-Frandsen K, Colhoun HM, et al. Semaglutide and cardiovascular outcomes in obesity without diabetes. New England Journal of Medicine. 2023;389(24):2221–2232. DOI: 10.1056/NEJMoa2307563. Ryan DH, Lingvay I, Colhoun HM, et al. Semaglutide effects on cardiovascular outcomes in people with overweight or obesity: SELECT study baseline characteristics. Obesity. 2023;31:111–122. ClinicalTrials.gov. Semaglutide Effects on Heart Disease and Stroke in Patients With Overweight or Obesity—SELECT. Trial registration NCT03574597.