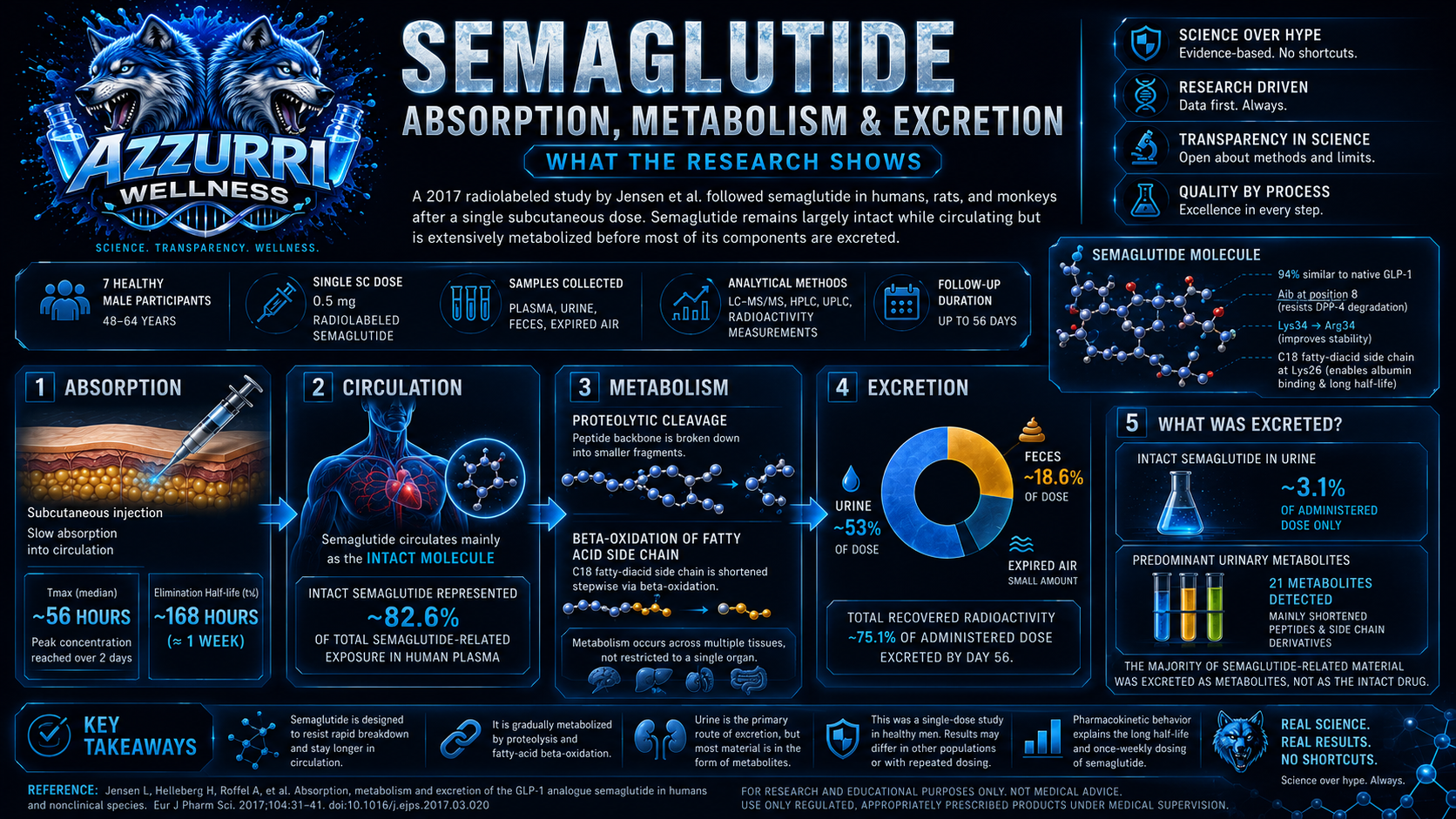
Semaglutide is a modified peptide designed to remain in circulation much longer than native glucagon-like peptide-1, or GLP-1. Understanding its clinical effects requires more than knowing that it activates the GLP-1 receptor. Researchers must also determine how quickly the molecule enters circulation, how long it remains present, what chemical changes it undergoes, and how its degradation products eventually leave the body. A 2017 study by Jensen and colleagues investigated these questions using radiolabeled semaglutide in healthy human participants, rats, and monkeys. The research provides a detailed picture of semaglutide absorption, metabolism, and excretion after a single subcutaneous dose. The central finding was: Semaglutide circulated mainly as the intact molecule but was extensively broken down before most semaglutide-related material was excreted. That distinction is important. Finding semaglutide-related material in urine does not mean that the kidneys simply filter and remove large amounts of unchanged semaglutide. The paper at a glance The human portion of the study included seven healthy men between 48 and 64 years of age. Each participant received one subcutaneous dose containing 0.5 mg of tritium-radiolabeled semaglutide. Researchers then collected and analyzed plasma, blood, urine, feces, and expired-air samples over an extended period. The researchers used several complementary techniques: Liquid chromatography–tandem mass spectrometry to measure intact semaglutide Radioactivity measurements to track semaglutide-related material HPLC and UPLC to separate metabolites High-resolution mass spectrometry to investigate metabolite structures The study also compared human findings with experiments conducted in rats and monkeys. This was an absorption, metabolism, and excretion study. It was not designed to measure weight loss, glucose control, long-term safety, or comparative treatment effectiveness. Why semaglutide lasts longer than native GLP-1
Native GLP-1 is rapidly degraded in circulation and has a half-life measured in minutes. Semaglutide was engineered with specific structural changes intended to reduce enzymatic degradation and slow systemic elimination. It retains approximately 94% structural similarity to native human GLP-1 but includes three important modifications: Alanine at position 8 is replaced with alpha-aminoisobutyric acid. Lysine at position 34 is replaced with arginine. Lysine at position 26 carries a spacer and C18 fatty-diacid side chain. The position-8 substitution reduces susceptibility to degradation by dipeptidyl peptidase-4, while the fatty-acid-containing side chain promotes albumin binding. Together, these changes help extend semaglutide’s circulation time. Albumin binding matters because it can reduce rapid renal filtration and create a circulating reservoir from which semaglutide is released gradually. Later population pharmacokinetic work found that semaglutide’s prolonged exposure was driven mainly by slow elimination and, to a smaller extent, delayed absorption. What did the study show about absorption? After the single subcutaneous injection, the median time to maximum plasma concentration was approximately 56 hours. This means that the highest measured plasma concentration was reached more than two days after administration. The geometric mean elimination half-life was approximately 168 hours, equivalent to about one week. These findings help explain the relatively gradual rise and prolonged decline in semaglutide concentration following subcutaneous administration. However, the time to maximum concentration should not be interpreted as a pure measurement of absorption alone. The observed concentration-time profile reflects several overlapping processes: Movement from the injection site into circulation Distribution in plasma and tissues Albumin binding Metabolic degradation Systemic elimination Later pharmacokinetic modelling estimated high subcutaneous bioavailability and confirmed that semaglutide’s long terminal half-life is driven primarily by slow disposition rather than exceptionally slow absorption alone. Radioactivity persisted longer than intact-drug measurements alone Semaglutide-related radioactivity remained detectable in plasma at the final sampling point, 56 days after administration. This does not mean that unchanged semaglutide remained at its original concentration for 56 days. The radioactivity measurements included intact semaglutide, metabolites, and some volatile labeled components. The half-life of intact semaglutide itself was approximately one week. This distinction illustrates why radiolabeled pharmacokinetic studies require careful interpretation: A radioactive signal shows that labeled material remains present. It does not automatically prove that the complete original molecule remains intact. What circulated in plasma? Intact semaglutide was the dominant semaglutide-related component in human plasma. Based on total exposure over time, intact semaglutide represented approximately 82.6% of the semaglutide-related material detected in human plasma. Six metabolite peaks were also identified, but each represented a relatively small fraction of total exposure. The largest metabolite peak represented 7.7% of total related exposure, but further analysis showed that this peak actually contained several coeluting components. These included a truncated semaglutide-derived peptide and several proposed semaglutide isomers. By samples collected after Day 28, intact radiolabeled semaglutide was the only semaglutide-related plasma component detected above the analytical threshold used in the study. The general interpretation is that semaglutide was comparatively stable while circulating. It was not immediately converted into one dominant circulating metabolite. How was semaglutide metabolized? The researchers identified two principal metabolic processes: 1. Proteolytic cleavage of the peptide backbone Proteolysis occurs when enzymes break peptide bonds within an amino-acid chain. Semaglutide’s peptide portion was gradually divided into smaller peptide fragments and amino-acid-related products. The most prominent characterized plasma metabolite included a truncated sequence missing the first 13 amino-acid residues. Semaglutide’s modified position 8 reduces susceptibility to DPP-4, but the molecule is not completely resistant to all peptide-degrading enzymes. The authors discussed neutral endopeptidase as a possible contributor to some observed cleavage patterns, although some supporting enzyme experiments cited in the article were exploratory and unpublished. 2. Beta-oxidation of the fatty-acid side chain Semaglutide contains a C18 fatty-diacid side chain that contributes to its prolonged albumin binding. The study found evidence that this side chain underwent sequential beta-oxidation. Beta-oxidation removes carbon units from fatty-acid structures in stages, producing progressively shorter side-chain derivatives. Two major urinary metabolites were identified as products containing the lysine-26 region and shortened C4 or C6 di-acid side chains. Each represented approximately 14% of the administered radioactive dose. The resulting picture is not one of a single metabolic cut. Semaglutide was gradually processed through a combination of peptide-backbone cleavage and fatty-side-chain shortening. Was semaglutide metabolized mainly in the liver? The study did not identify one specific organ as the exclusive site of semaglutide metabolism. The authors concluded that semaglutide was metabolized across tissues and that its degradation pathways were not confined to a single organ. Proteolytic enzymes are distributed in plasma and multiple tissues, while beta-oxidation is a widespread biological process. This finding should not be interpreted as proof that every tissue contributes equally. The radiolabeled study characterized circulating and excreted products but did not calculate a separate metabolic rate for each human organ. A more accurate statement is: The evidence did not support one exclusive organ-specific pathway for semaglutide breakdown. How was semaglutide-related material excreted? The researchers recovered approximately 75.1% of the administered radioactive dose from human excreta. The major routes were: Approximately 53% recovered in urine Approximately 18.6% recovered in feces A smaller amount detected through expired air Excretion was slow and was close to completion by approximately Day 56, consistent with the molecule’s long half-life. Urine was therefore the largest route for elimination of semaglutide-related radioactivity. But this result requires an important qualification. Most urinary material was not intact semaglutide Only approximately 3.1% of the administered dose was recovered in human urine as intact semaglutide. Twenty-one additional metabolites were detected in urine. Intact semaglutide was not detected in human feces. Instead, seven metabolite components were found, each representing no more than a small proportion of the administered dose. The correct interpretation is therefore: Urinary excretion was the principal route for semaglutide-derived material, but the material was predominantly metabolic degradation products rather than unchanged semaglutide. This is different from saying that semaglutide is simply cleared intact by the kidneys. What did the animal comparisons show? Intact semaglutide was also the major circulating component in rats and monkeys. The overall metabolite profiles appeared broadly similar across humans, rats, and monkeys, with proteolytic cleavage and fatty-acid beta-oxidation occurring across species. The researchers reported no major human-specific circulating metabolite that exceeded the thresholds discussed for additional safety investigation. Total recovered radioactivity was: 75.1% in humans 72.1% in rats 58.2% in monkeys The lower monkey recovery was partly related to sample collection ending while semaglutide-related material was still being excreted. Similarity across animal and human metabolite profiles was relevant during development because major human-specific metabolites can require additional investigation. However, similar chromatographic profiles do not mean animal metabolism perfectly predicts every human clinical response. Animal comparisons are supporting evidence, not substitutes for adequately powered human studies. Why did researchers use radiolabeled semaglutide? The researchers attached a tritium label to the fatty-diacid region of semaglutide. This allowed them to track semaglutide-related material even after the original molecule had been broken into smaller metabolites. The selected labeled carbon–hydrogen bond was reported to be chemically stable under the conditions evaluated, reducing the chance that the label would be lost randomly before metabolic processing occurred. Radiolabeling is useful because ordinary assays may detect only the intact drug or a limited group of known metabolites. A radioactive tracer can reveal a wider mass-balance picture. However, the location of the label is also a limitation. Because the isotope was attached to the fatty-acid side chain, the study was particularly suited to tracking that modified region. The authors stated that radiolabeling of the entire peptide sequence was outside the study’s scope. It should therefore not be described as a complete atom-by-atom map of every possible peptide-backbone fragment. What this study does—and does not—prove The study supports these conclusions Semaglutide reached peak plasma concentration gradually after subcutaneous administration. Intact semaglutide dominated the circulating plasma profile. Its measured half-life was approximately one week. The molecule underwent proteolytic peptide cleavage and fatty-side-chain beta-oxidation. Urine was the main route for excretion of semaglutide-related material. Only a small proportion of the administered dose was excreted in urine as intact semaglutide. Human, rat, and monkey metabolite patterns appeared broadly comparable. The study does not establish Long-term treatment effectiveness Weight-loss outcomes Comparative safety against other medications Metabolism after chronic repeated administration Pharmacokinetics in every patient population The behaviour of oral semaglutide The behaviour of unverified or non-pharmaceutical semaglutide products These boundaries matter because the human study involved only seven healthy men receiving a single subcutaneous dose. Study limitations and funding The human sample was small and demographically narrow. All seven participants were healthy adult men, mostly in their 50s and early 60s. The findings therefore cannot, by themselves, establish identical pharmacokinetics in women, younger adults, people with type 2 diabetes, people with obesity, patients with multiple health conditions, or individuals receiving repeated doses. The study also used one 0.5 mg subcutaneous dose. Its results should not be transferred directly to oral administration or every possible dosing schedule. The clinical and preclinical research was funded by Novo Nordisk. Several authors were affiliated with Novo Nordisk or the contracted research organization, and manufacturer-funded editorial support was acknowledged. Funding does not automatically invalidate the findings, but it should be disclosed when interpreting the evidence. Later pharmacokinetic analyses involving larger datasets supported a predictable, long-duration semaglutide profile, but those analyses were also manufacturer-funded and included authors employed by or holding stock in Novo Nordisk. The Azzurri Wellness perspective This paper demonstrates why peptide research must look beyond the name of the molecule. Semaglutide’s pharmacokinetic behaviour reflects several interconnected design features: Resistance to rapid enzymatic degradation Reversible albumin binding Slow systemic elimination Gradual proteolytic cleavage Metabolism of its fatty-acid side chain Excretion of predominantly degraded products The study also demonstrates why phrases such as “renal clearance” can be misleading without analytical context. Semaglutide-related radioactivity was found mainly in urine, but only a small part was unchanged semaglutide. Chromatography, radiodetection, and mass spectrometry were required to distinguish the intact molecule from its metabolites. The route of excretion does not, by itself, reveal the chemical form being excreted. Frequently asked questions Is semaglutide excreted unchanged in urine? Only to a limited extent. The study found that intact semaglutide represented approximately 3.1% of the administered human dose in urine. Most urinary semaglutide-related material consisted of metabolites. Does the liver completely metabolize semaglutide? The study did not identify the liver as the sole metabolic organ. The authors concluded that proteolysis and fatty-side-chain metabolism were not confined to one specific organ. What is semaglutide’s half-life? In this single-dose study, the geometric mean half-life was approximately 168 hours, or about one week. What was the main substance circulating in plasma? Intact semaglutide was the main circulating component and represented approximately 82.6% of total semaglutide-related plasma exposure in the human analysis. How is semaglutide broken down? The study identified proteolytic cleavage of the peptide backbone and sequential beta-oxidation of the C18 fatty-diacid side chain as major metabolic pathways. Does this paper prove semaglutide’s weight-loss effectiveness? No. This was an absorption, metabolism, and excretion study. It was not designed to evaluate weight-loss efficacy or long-term treatment outcomes.
References Jensen L, Helleberg H, Roffel A, van Lier JJ, Bjørnsdottir I, Pedersen PJ, et al. Absorption, metabolism and excretion of the GLP-1 analogue semaglutide in humans and nonclinical species. European Journal of Pharmaceutical Sciences. 2017;104:31–41. DOI: 10.1016/j.ejps.2017.03.020. Lau J, Bloch P, Schäffer L, Pettersson I, Spetzler J, Kofoed J, et al. Discovery of the once-weekly glucagon-like peptide-1 analogue semaglutide. Journal of Medicinal Chemistry. 2015;58(18):7370–7380. DOI: 10.1021/acs.jmedchem.5b00726. Overgaard RV, Delff PH, Petri KCC, Anderson TW, Flint A, Ingwersen SH. Population pharmacokinetics of semaglutide for type 2 diabetes. Diabetes Therapy. 2019;10:649–662. DOI: 10.1007/s13300-019-0581-y.